
Scaling
Growing a Private Medical Practice: The Complete Scale & Exit Guide for Practice Owners (2026)

Written by: Tanaka Chamisa
How to grow a private medical practice in the UK, from referral strategy and multi-site scaling to governance infrastructure and maximising your exit valuation.
You didn't spend years in training, build a patient base from scratch, and navigate the complexities of CQC registration to stay still.
Whether your goal is to scale to multiple sites, attract private equity interest, or build a practice that commands a premium sale price when the time is right, the decisions you make in the next 12 to 36 months will determine the outcome.
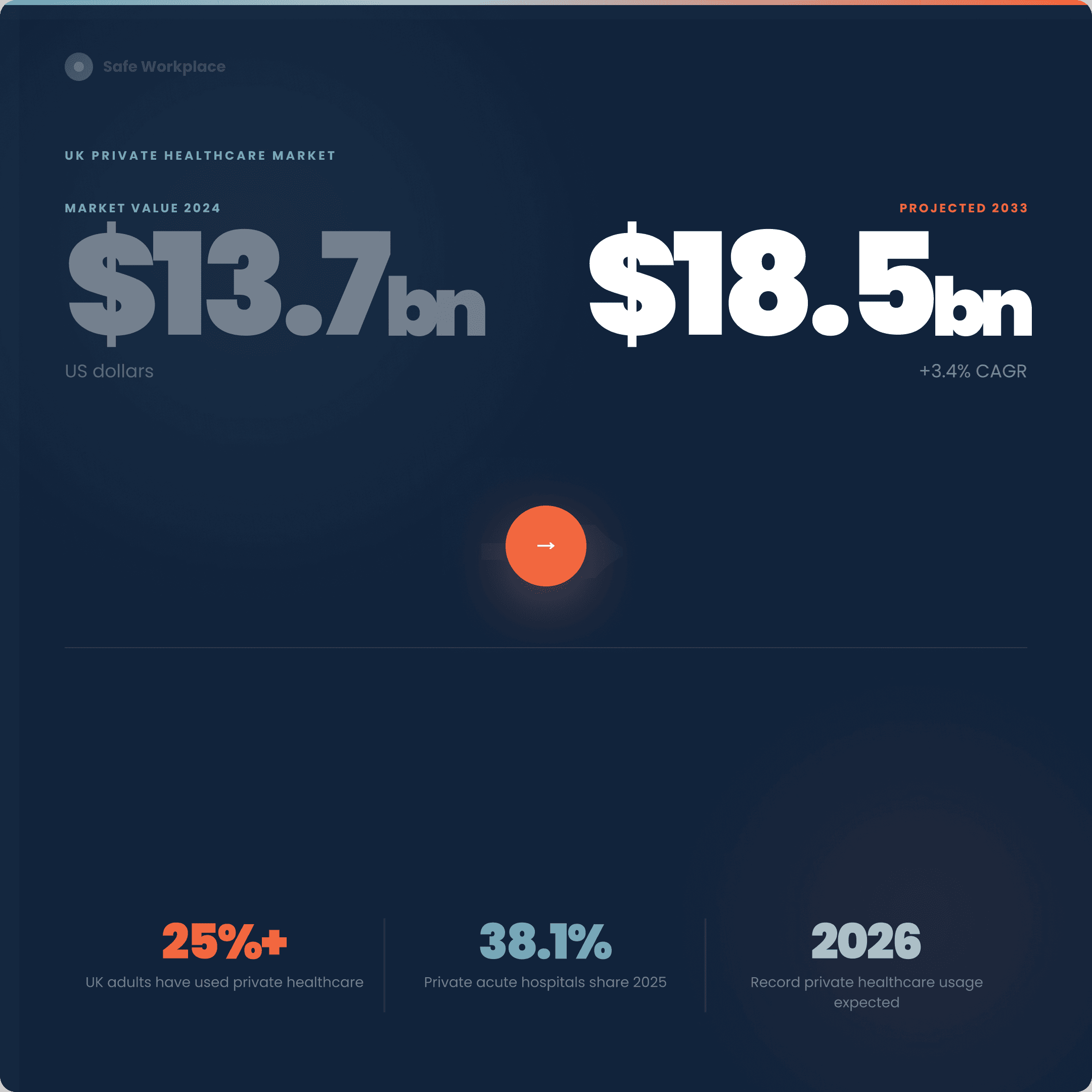
The UK private healthcare market was valued at US$13.75 billion in 2024 and is projected to reach US$18.56 billion by 2033, growing at a compound annual rate of 3.4%.
Analysts expect private healthcare usage to reach record levels by 2026 as patients look for reliable alternatives to NHS waiting lists. The market conditions have rarely been more favourable for practice owners with ambition.
But ambition without infrastructure is expensive. The practices that scale cleanly and exit well are not necessarily the ones with the most patients or the highest revenue. They are the ones with the most defensible operations:
Consistent governance
Documented processes
Clean compliance records
Evidence trails that hold up under scrutiny
Whether that scrutiny comes from a CQC inspector or an acquirer's due diligence team, the underlying requirement is identical.
This guide covers both sides of that equation. The growth strategies that build a scalable private practice, and the governance and compliance foundations that make that practice worth buying.
Understanding the Market You're Growing Into
The self-pay revolution
Approximately 33% of UK adults have now used private healthcare services, with mental health services seeing particularly strong growth. The driver is well understood: NHS waiting times have pushed patients who can afford an alternative to seek one.
But the profile of that patient is changing. Historically, private healthcare was the preserve of corporate PMI and high-net-worth individuals. The majority of private care patients use private medical insurance policies, with just 20% paying directly out of their own pockets. That ratio is shifting, and it matters for how you price, package, and position your services as you scale.
Self-pay patients have different expectations from insured patients. They are more price-sensitive but also more demanding around transparency, speed, and experience.
They compare you not just to other private providers but to the entire service economy. Building a scalable practice in 2026 and beyond means meeting both audiences without diluting either.
The NHS adjacency opportunity
The boundary between NHS and private care is becoming more flexible. To meet rising demand, the NHS is working closely with private providers to expand capacity for diagnostics, elective surgeries, and specialist treatment.
For practice owners, NHS outsourcing contracts represent a route to revenue predictability that pure private practice cannot offer. They also represent a route to scale, institutional contracts require the kind of governance infrastructure that small practices rarely have, which means getting your compliance foundations right is not just a regulatory obligation, it is a commercial differentiator.
The Seven Growth Levers for a Private Medical Practice
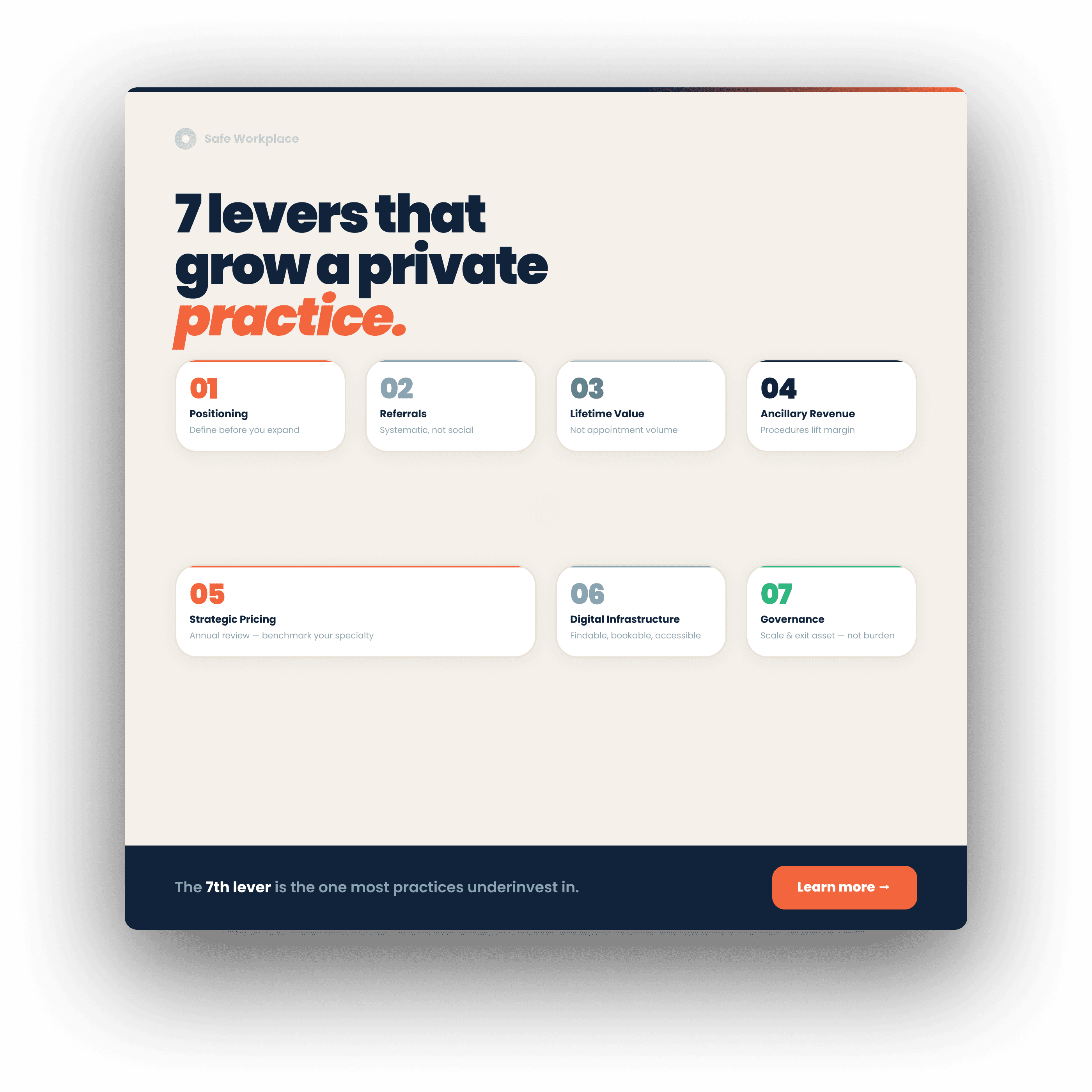
1. Clarify your positioning before you expand
The most common scaling mistake in private practice is attempting to grow before the positioning is clear. Adding services, opening a second site, or hiring additional clinicians into a practice that lacks a distinct identity creates operational complexity without creating a competitive advantage.
Your positioning answers three questions:
Who specifically you serve
What outcome you deliver for them
Why a patient should choose you over an equivalent alternative
A specialist fertility clinic, a sports medicine practice, and a general private GP practice all serve different patients with different decision drivers. Your marketing, pricing, referral relationships, and even your governance infrastructure should follow from that positioning, not precede it.
2. Build your referral infrastructure systematically
Successful private practices have a distinct identity and positioning. But identity without referral relationships is invisible. The most cost-effective growth lever for most private practices is a structured programme of GP and specialist referral relationships, not occasional networking, but a deliberate, tracked system of relationship-building with the primary care and secondary care clinicians whose patients match your ideal patient profile.
This means knowing which GPs are within your catchment area, which of their patients are most likely to need your services, and what information those GPs need to refer with confidence. Most practices manage this informally and inconsistently. Building a referral CRM — even a simple one — transforms a social activity into a scalable growth engine.
3. Optimise for lifetime patient value, not appointment volume
Scaling a practice by increasing appointment volume alone produces diminishing returns. The unit economics worsen as you add capacity — more rooms, more clinical staff, more administrative overhead — without a corresponding increase in margin per patient.
The practices that scale most profitably focus on patient lifetime value. A patient who attends once for a consultation is worth less than a patient who returns annually, refers their family members, and subscribes to a health monitoring service. Building the conditions for high lifetime value, excellent clinical outcomes, proactive follow-up, seamless communication, and a patient experience that feels different from both NHS and transactional private care — is the single most durable growth strategy available.
4. Develop ancillary revenue streams
Procedure-rich practices command premium valuations at exit. The logic is straightforward: diagnostic and treatment services generate higher margins than consultations alone, and they create stickier patient relationships. If your practice currently generates revenue primarily through consultation fees, expanding into diagnostics, aesthetic treatments, health screening packages, or chronic disease management programmes diversifies your income and increases average revenue per patient.
The key constraint is clinical coherence. Ancillary services that sit naturally within your clinical positioning strengthen it. Services that feel like a different business weaken your brand and create operational complexity without proportionate commercial return.
5. Price strategically, not reactively
Most private practice owners set their fees at the start of their practice and adjust them infrequently, usually in response to financial pressure rather than market analysis. This is one of the most significant value leakage points in the sector.
Pricing in private healthcare is not simply about what the market will bear. It is a signal of clinical quality, practice positioning, and patient experience. Underpriced services attract price-sensitive patients who are harder to retain and less likely to refer. Properly priced services attract patients whose expectations match what you can sustainably deliver.
Review your fee schedule annually. Benchmark against comparable practices in your geography and specialty. And price your most distinctive services, the ones where you have genuine clinical expertise or exceptional outcomes, at a premium that reflects their actual value.
6. Build the digital infrastructure your growth requires
More patients are choosing to self-fund care, and expectations around speed, transparency and quality are rising. At the same time, practices are doing more, offering more services, more coordination, producing more data and requiring more admin.
A practice that cannot be found, booked, or communicated with digitally is capping its own growth. This does not mean expensive bespoke technology. It means a clear, patient-facing website with genuine clinical credibility; online booking that works on mobile; automated appointment reminders and follow-up communications; and a patient portal that gives patients access to their records and results without requiring a phone call.
The practices that scale fastest in 2026 are those that have separated the clinical experience from the administrative friction. Patients should feel the quality of your clinical care from the first search result, not only from the moment they sit in your consultation room.
7. Governance as a growth asset and not a compliance burden
This is the lever most practice owners underinvest in, and the one that has the greatest impact on both scale and exit value.
The CQC's Single Assessment Framework has been around for over a year now, and this has set the scene for continuous, evidence-led assessment, rather than a single periodic inspection.
Practices are increasingly aware that compliance comes from being able to show how things work day to day rather than gearing up for a one-off moment.
The governance infrastructure that satisfies CQC under the Single Assessment Framework is identical to the governance infrastructure that satisfies an acquirer's due diligence team. Documented incident management. Clear policies with tracked acknowledgement. Risk registers that are maintained continuously, not assembled before an inspection. Audit trails that show how your practice identifies problems, acts on them, and demonstrates improvement over time.
This is not just a regulatory obligation. It is the evidence base that makes your practice scalable and sellable.
The Compliance Foundation That Makes Scale Possible
Growing a private medical practice without adequate governance infrastructure is like building on sand. The growth looks impressive until the pressure increases, a CQC inspection, an adverse patient event, a due diligence process and the foundations show.
What CQC actually looks for in a scaling practice
If a process lives mainly in someone's head, inbox or on a spreadsheet, it creates both risk and pressure. This is the core diagnostic question for any practice considering growth: could your governance infrastructure survive the addition of a second clinician, a second site, or a significant increase in patient volume?
The CQC's five key questions; Safe, Effective, Caring, Responsive, and Well-led, do not become easier to satisfy as you grow.
They become harder. A solo practitioner can maintain clinical quality through personal oversight. A multi-clinician, multi-site practice requires systems that produce consistent outcomes regardless of which clinician is on duty and regardless of which site the patient attends.
Well-led, which accounts for 31% of Requires Improvement ratings nationally, is the domain that exposes governance weaknesses most clearly at scale.
Inspectors ask: Does leadership have real-time visibility of what is happening across the practice? Is there a functioning system for capturing concerns, incidents, and feedback? When something goes wrong, is there evidence of learning, not just of response?
Building governance infrastructure that scales
The governance infrastructure a growing private practice needs covers five interconnected areas:
Incident and concern management
Every incident, near miss, and patient concern should be captured in a structured system, not a shared inbox or a spreadsheet, with clear workflows for investigation, escalation, and closure. As your practice grows, the volume of incidents will increase. The system needs to handle that volume without creating an administrative burden on clinical staff, and it needs to produce trend data that allows leadership to identify patterns before they become serious problems.
Policy management
Every clinical and operational policy in your practice should be documented, version-controlled, and actively acknowledged by the staff it applies to. Policies that sit in a folder on a shared drive are not governance, they are paper. Governance is the evidence that the right people have read, understood, and are acting on current policy. At scale, with multiple clinicians and multiple sites, managing this without a dedicated system becomes effectively impossible.
Risk management
Your risk register should be a live document that reflects the current risk profile of your practice, not an annual exercise. Risks should be scored, owned, reviewed on a defined schedule, and connected to the mitigating actions that reduce them. When a new service is added, a new clinician joins, or a new site opens, the risk register should be updated to reflect the changed profile.
Audit and quality assurance
Clinical audit is the mechanism by which a practice demonstrates that its care is evidence-based and continuously improving. For CQC, it is also the most powerful evidence of a learning culture. A practice that conducts regular, structured audits, and can show how audit findings have translated into changed practice, is a practice that satisfies the CQC's Well-led quality statements and a practice that an acquirer can underwrite with confidence.
Training and competency management
Every member of clinical and administrative staff should have a training record that is current, complete, and connected to the policies and procedures they are expected to follow. Training that is not evidenced is training that does not exist in the eyes of a regulator or an acquirer.
How Safe Workplace connects these five areas
Most private practices manage these five areas in separate systems or do not manage them systematically at all. Incidents are logged in one place, policies stored in another, training records in a third, and audit findings in a spreadsheet that gets updated before inspections.
Safe Workplace was built specifically for regulated healthcare providers who need these five areas to work as one connected system.
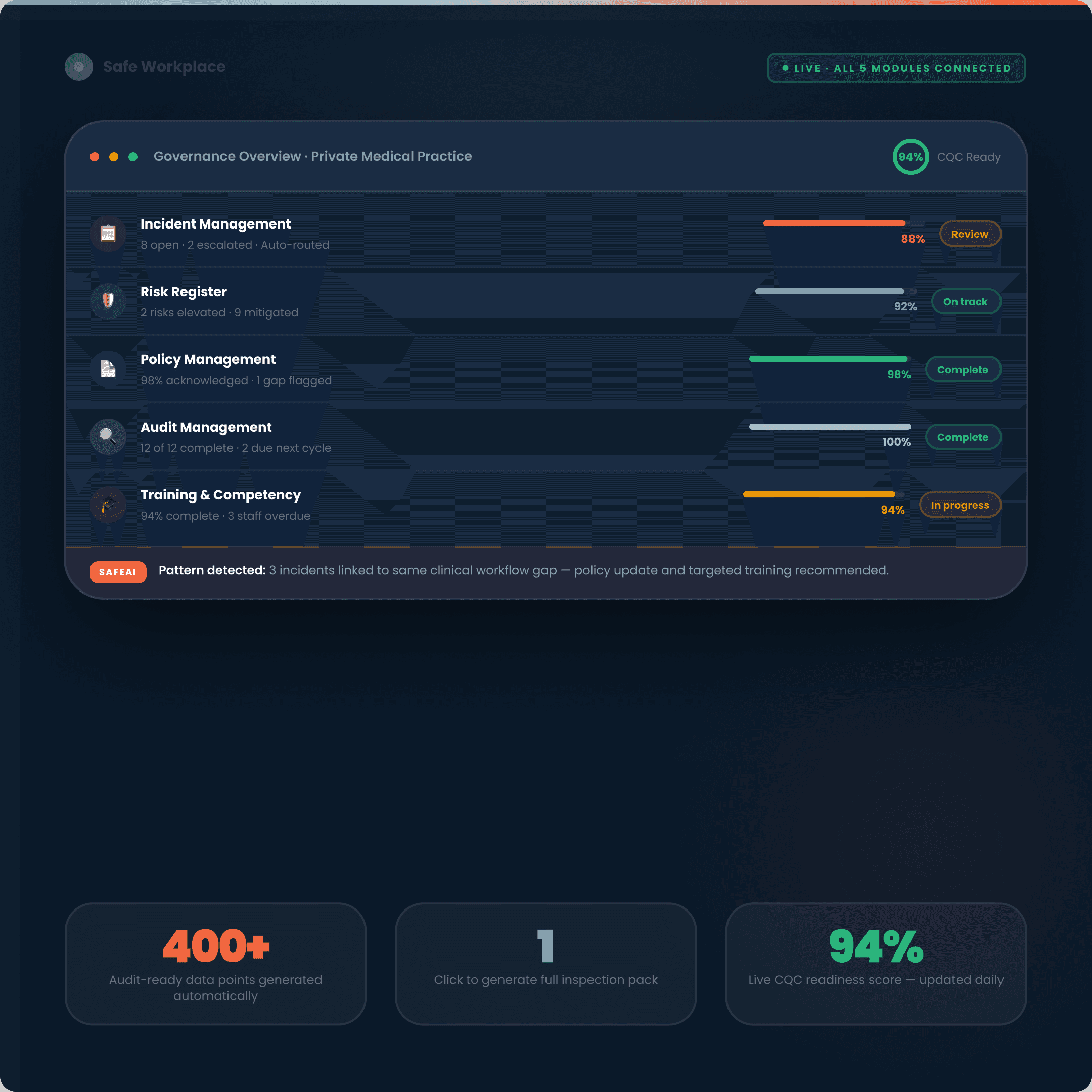
When an incident is logged, it automatically maps to the relevant compliance frameworks. When a policy is updated, staff receive an acknowledgement request linked to the reason for the change. When an audit finding identifies a gap, an action is created, assigned, and tracked to completion — with the evidence of that closure attached to the original finding.
The result is a live compliance readiness score that reflects the actual governance status of your practice at any given moment — not the status as of your last inspection preparation exercise. When CQC arrives, or when an acquirer begins due diligence, the evidence pack is one click away.
Scaling to Multiple Sites
Opening a second site is the inflection point at which most private practices discover the limits of their existing governance infrastructure. The problems that were manageable at one site, inconsistent incident reporting, policies that exist but are not consistently applied, training records that are out of date, become significant operational and regulatory risks at two or three sites.
The governance checklist before you open a second site
Before committing to a second location, your governance infrastructure should be able to answer yes to the following:
Does your incident management system capture incidents from any location in real time? Can leadership see the full picture across all sites without compiling manual reports?
Are your policies consistently applied across all clinical staff? Do you have evidence of acknowledgement, not just circulation?
Could you generate a compliance readiness report for each site independently, as well as consolidated across the whole practice, in under an hour?
If the answer to any of these is no, the second site will add regulatory risk faster than it adds revenue. Get the infrastructure right at one site first. Then scale it.
The staffing and governance challenge at scale
Managing compliance across multiple locations, departments, or systems becomes increasingly difficult as healthcare organisations scale. Scalable compliance software ensures consistency across all operations, making growth smoother and less risky.
The most common failure mode for multi-site private practices is inconsistency, not incompetence. Individual clinicians deliver excellent care. But without systems that standardise how incidents are reported, how policies are applied, and how quality is monitored, the clinical experience varies by location in ways that create both patient safety risk and reputational risk.
The practices that scale most successfully establish governance systems that work the same way regardless of which site a patient attends or which clinician they see. Consistency at scale is the product of systems, not of individual excellence.
Building for Exit: What Acquirers Actually Buy
Practice owners should begin preparing for a sale at least 2 to 3 years in advance to maximise valuation and ensure a smooth transition. Most do not. And the practices that come to market without adequate preparation consistently achieve lower multiples than those that have built with exit in mind from the start.
The valuation fundamentals
Most practices sell for 3 to 6 times EBITDA, though specialty, profitability, growth trajectory, and market conditions significantly impact multiples. Specialty practices command significantly higher multiples in 2025 to 2026 due to scarcity, higher barriers to entry, and superior reimbursement rates. Surgical specialty practices sell for approximately 26% premium compared to primary care practices.
But the multiple is only half the equation. The EBITDA calculation matters as much as the multiple applied to it. Owner compensation resets, one-time expenses, and related-party adjustments all affect the normalised EBITDA that a buyer will underwrite.
A practice generating £500,000 of revenue with an owner who draws a below-market salary may show higher EBITDA than the same practice with a market-rate salary, but a buyer will adjust for this, and a practice that cannot clearly document and defend its normalised EBITDA will leave value on the table.
What moves the multiple up
Early preparation, accurate financials, growth plans, and compliance readiness, remains the most reliable path to top-quartile outcomes.
The factors that consistently command premium multiples in private practice transactions:
Revenue diversification: Practices dependent on a single revenue stream, consultation fees from a single clinician, are valued at a discount to those with multiple income sources, multiple clinicians, and a mix of self-pay, PMI, and NHS-funded activity.
Clinical independence from the owner: A practice where patients attend because of the individual reputation of the owner-clinician is worth significantly less than one where patients attend because of the practice brand and clinical team. Buyers are underwriting the future earnings of the practice, not its historical relationship with a specific clinician. The more transferable the patient relationships, the higher the multiple.
Documented governance and compliance: Many medical practices have significant untapped growth potential that can be unlocked with the resources and expertise of a larger organisation. Acquiring your practice could provide them with a foothold in a new geographic market, access to a new patient population, or the ability to offer a new service line. Buyers who see this potential will pay a premium — but only if the due diligence process confirms that the practice's operations are clean, documented, and transferable. A practice with poor governance records, unresolved CQC concerns, or undocumented processes will be discounted aggressively regardless of its revenue profile.
Growth trajectory: Buyers price the future, not the past. A practice growing at 15% per annum with a clear pipeline of new referral relationships and a documented growth strategy will attract higher multiples than a static practice with the same EBITDA.
The compliance-valuation connection
This is the point most practice owners miss. Your CQC compliance record is not just a regulatory matter. It is a commercial matter. An acquirer performing due diligence on your practice will examine your CQC inspection history, your incident management records, your policy documentation, and your governance audit trail with the same scrutiny that a regulator would.
A practice with a clear compliance history, documented incidents, evidenced improvements, current policies with tracked acknowledgement, and a live risk register, is a practice that an acquirer can underwrite with confidence. The due diligence process is shorter, the conditions attached to the sale are fewer, and the price achieved is higher.
A practice with gaps in its governance record, incidents managed informally, policies that exist but are not consistently followed, a risk register that was last updated before the previous CQC inspection — will face extended due diligence, price chips, or conditions that delay or undermine the transaction.
Building Safe Workplace into your practice two or three years before you plan to exit is not just about CQC compliance. It is about building the governance evidence base that makes your practice sellable at a premium.
The Practice Growth Audit: Your Free Self-Assessment Tool
Before you can scale or exit effectively, you need to know where your practice currently stands. The Safe Workplace Practice Growth Audit is a structured self-assessment covering the five governance and operational areas that most directly affect your ability to scale and your valuation at exit.
What the audit covers:
Governance readiness score: How well-structured is your incident management, risk register, policy management, and audit activity? Would your current governance infrastructure survive a CQC inspection tomorrow?
Clinical independence score:How dependent is your practice's revenue on your personal clinical relationships? What would happen to revenue if you were unable to work for three months?
Operational scalability score: Are your processes documented and consistently applied? Could a new clinician or site be onboarded using your existing systems?
Financial clarity score: Can you produce a normalised EBITDA calculation for your practice? Do you have three years of clean management accounts?
Growth trajectory score: Do you have a documented referral development plan? Are you tracking patient lifetime value and referral sources?
Frequently Asked Questions
How long does it take to grow a private medical practice to a point where it is saleable?
The honest answer is three to five years from a standing start, assuming you are building deliberately toward a sale from the beginning. The two most time-consuming elements are building a patient base that is not dependent on your personal clinical reputation and establishing a governance and compliance record that holds up under acquirer scrutiny. Practices that begin building their compliance infrastructure from the point of CQC registration, rather than treating it as a reactive exercise, consistently achieve stronger valuation outcomes than those that retrofit governance structures in the year before going to market.
What is a realistic valuation multiple for a private medical practice in the UK?
Most practices sell for 3 to 6 times EBITDA, though specialty, profitability, growth trajectory, and market conditions significantly impact multiples. Specialty practices in high-demand areas — cardiology, gastroenterology, ophthalmology, command premiums above this range. General practice and primary care typically sit at the lower end. The multiple applied to your normalised EBITDA will also be affected by revenue diversification, clinical independence from the owner, and the quality of your governance and compliance documentation.
Does CQC compliance actually affect the sale price of a private practice?
Yes, directly. An acquirer's due diligence process will review your CQC inspection history, your incident management records, and your governance documentation. A practice with gaps, outstanding concerns, or informal processes will face price reductions, extended due diligence timelines, or transaction conditions that effectively reduce the net proceeds of the sale. A practice with a clean compliance record and well-documented governance infrastructure reduces the acquirer's perceived risk and commands a correspondingly higher price.
When should I start thinking about exit strategy?
Practice owners should begin preparing for a sale at least 2 to 3 years in advance to maximise valuation and ensure a smooth transition. In practice, the decisions you make about governance infrastructure, clinical team composition, revenue diversification, and practice positioning from the point you start your practice will determine the exit options available to you. The practices that achieve the strongest exit outcomes are those that built with exit in mind from the beginning — not those that retrofitted a strategy when the time came.
What is the difference between a trade sale and a private equity exit for a private medical practice?
A trade sale involves selling your practice to another healthcare provider, a hospital group, a larger practice, or a corporate consolidator. A private equity exit involves selling a majority or minority stake to a PE firm that will use your practice as a platform for further acquisition and growth. The 2025 to 2026 environment demands more sophisticated approaches than simple multiple applications — buyers challenge EBITDA adjustments aggressively, and regulatory scrutiny continues intensifying across healthcare transactions. For most independent practice owners, a trade sale is the most straightforward exit route. PE exits typically require larger scale, stronger EBITDA, and a management team that can operate independently of the founding clinician.
How does Safe Workplace help a private medical practice prepare for CQC inspection and exit?
Safe Workplace connects your incident management, policy management, risk register, audit activity, and training records in a single platform so your compliance evidence builds continuously rather than being assembled before inspections or due diligence.
The result is a live compliance readiness score, a governance audit trail that satisfies CQC's Single Assessment Framework requirements, and an evidence base that an acquirer can review with confidence.
Practices using Safe Workplace have walked into CQC inspections with 400+ audit-ready data points generated automatically through their day-to-day operations.


